ECR 2017 / C-1966
Orbitofacial Trauma : A Systematic Approach to CT Imaging
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-1966
Type:
Educational Exhibit
Keywords:
Image verification, Fractal analysis, CT, Head and neck, Eyes, Emergency
Authors:
N. Garrouche, M. Gaha, M. M. Mestiri, N. Arifa, N. Mama, K. Mrad Dali, H. Jemni; Sousse/TN
DOI:
10.1594/ecr2017/C-1966
 Sphenoid, Zyg) Zygomatic, Max) Maxillary, Lac)Lacrimal, Eth)Ethmoidal, Fr) Frontal, Pal) Palatine References: cyber-sight(edited)")
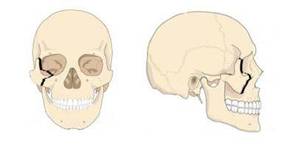
Fig. 1:
Bony orbit anatomy: Sph) Sphenoid, Zyg) Zygomatic, Max) Maxillary,...

Fig. 2:
Axial and coronal CT views showing the intraorbital normal anatomy :
AC:...

Fig. 3:
Bone anatomy of the Orbit on CT MPR:
1.Medial wall
2.Orbital...

References: http://www.skullanatomy.info")
Fig. 4:
Craniofacial skeleton showing The orbit medial wall anatomy which articulates...
Axial nonenhanced CT image shows the nomal anatomy of lamina papyracea
b)Coronal view shows the nasolacrimal canal (arrow head)
References: Radiology department Sahloul University hospital")
Fig. 5:
Important structures on medial wall .
a)Axial nonenhanced CT image shows the...

Fig. 6:
The orbital floor on 3D reformation CT image

Fig. 7:
The orbital floor, with the infraorbital groove on coronal and axial CT...

Fig. 8:
Non enhanced CT image with Axial view showing the Lateral orbital wall ,...
 , the Inferior orbital Fissure(IOF) , Nasofrontal suture(*), Zygomatico-frontal suture (**), Zygomatico-temporal suture (***).
References: www.radiologyinthai.com")
Fig. 9:
3D CT anterior view showing: the Superior orbitalFissure (SOF) , the Inferior...

Fig. 10:
Schematic illustration of the orbital roof
 with alignment of the zygoma and sphenoid along the lateral orbital wall (blue line). Superior orbital fissure (yellow arrow)
Optical canal (orange arrow).
References: Radiology department Sahloul University hospital")
Fig. 11:
Axial nonenhanced CT images showing the normal anatomy of the orbital apices...

Fig. 12:
3D reformation CT showing the supraorbital notch which is the location of the...
")
Fig. 13:
Orbital skeleton showing the The annulus insertion along the
orbital apex,...

Fig. 14:
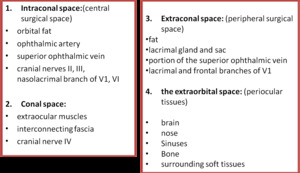
Schematic illustration of the the surgical spaces of the orbit on axial view,...

References: Radiology department Sahloul University hospital")
Fig. 15:
Axial CT images showing dislocated lens (arrows)

Fig. 16:
Coronal CT view showing Right orbital floor fracture: small defect in the...

References: Radiology department Sahloul University hospital")
Fig. 17:
Coronal CT view showing Blow-out fracture of the orbital floor : depression...
 Blow out Fractures of the medial orbital wall on non-enhanced coronal CT image .
(b)the axial view show the displacement of the lamina papyracea with blood acumulation in adiacent ethmoidal cells (cross)
References: Radiology department Sahloul University hospital")
Fig. 18:
(a) Blow out Fractures of the medial orbital wall on non-enhanced coronal ...
 Coronal CT scan showing a medial wall blow-out fracture of the left orbit (white arrows). (b) Orbital fat is seen to herniate into the defect (yellow arrow). The cross-sectional appearance of the muscle has changed from flattened to ovoid, indicating entrapment because of disruption of thefascial support
References: Radiology department Sahloul University hospital")
Fig. 19:
ca) Coronal CT scan showing a medial wall blow-out fracture of the left orbit...
 and Coronal (b) nonenhanced CT image show fractures of the zygomatic bone (red arrows)that forms external wall of orbit asssociated with medial wall and orbital floor fractures (yellow arrows). the right maxillary sinus is completely opacified. References: Radiology department Sahloul University hospital")
Fig. 20:
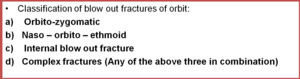
Orbito zygomatic fracture : Fractures of the orbital walls with zygomatic...
 axial CT image and (b) 3D reformation showing ZMC fracture
with frontal and sphenoid fracture.
References: Radiology department Sahloul University hospital")
Fig. 21:
(a) axial CT image and (b) 3D reformation showing ZMC fracture
with frontal...
 Axial (b)coronal nonenhanced CT image, (c) 3D-reformatted CT image. fracture of the right frontal sinus table that involves the right orbital roof with minimal bone displacement.
References: Radiology department Sahloul University hospital")
Fig. 22:
Orbital roof fracture. (a) Axial (b)coronal nonenhanced CT image, (c)...

Fig. 23:
Axial CT images showing NOE fracture with :
nasal fracture
Lateral wall...

Fig. 24:
Complex NOE fracture with Fractures of the orbital floor on axial ,coronal ...
. References: Radiology department Sahloul University hospital")
Fig. 25:
Optic nerve injury on axial CT view showing a right apex fracture
With a bone...

Fig. 26:
Comminuted fracture involving the medial walls of both orbits and frontal...

Fig. 27:
Post traumatic Interruption in Internal carotid artery supra cavernous